Fungal lung disease, particularly aspergilloma, poses a significant health challenge that demands expert medical attention. Dr Pallavi Purwar offers cutting-edge surgical treatment for Aspergilloma / Fungal Lung Disease, offering hope to patients grappling with this complex condition. As amongst the top fungal pneumonia treatment doctors in Delhi – Dr Pallavi Purwar is at the forefront of combating aspergillosis, employing advanced surgical techniques and comprehensive care strategies to address the fungus ball in lung and associated complications.
Dr Pallavi offers expert aspergilloma surgery in Delhi with revolutionised latest surgical approach to treating this stubborn fungal infection. Dr Pallavi Purwar also specialises in pulmonary fibrosis treatment in Delhi utilising state-of-the-art procedures to remove aspergillomas effectively, improving patient outcomes. As a skilled surgeon, Dr Pallavi focus on the timely implementation of anti-fungal therapy (as per individual patient needs), recognising its crucial role in managing the disease. With a combination of surgical expertise and medical management, healthcare facilities under Dr Pallavi are setting new standards in aspergillosis treatment, offering patients a chance at better lung health and improved quality of life.
Comprehensive Diagnosis of Aspergilloma
Clinical Presentation
Predisposing Conditions
- Former TB cavity
- Advanced sarcoidosis
- Pneumoconiosis
- Bullous emphysema
- Congenital cyst
- Acute/chronic infections
- Bronchiectasis
- Lung abscess
- Malignant Lesions
- Pulmonary infarct
- Postradiation pulmonary cavity
- Radiofrequency ablation
- Ankylosis spondylitis
Symptoms
- Haemoptysis
- Pneumothorax
- Cough
- Fever
- Weight loss
- Sputum
- Chest pain
- Dyspnea
- Asymptomatic
Aspergilloma may manifest as an asymptomatic radiographic abnormality in patients with preexisting cavitary lung disease due to conditions like sarcoidosis, tuberculosis, or other necrotising pulmonary processes. In patients with HIV disease, aspergilloma can occur in cystic areas resulting from prior Pneumocystis jiroveci pneumonia. Of patients with aspergilloma, 40-60% experience hemoptysis, which may be massive and life-threatening. Less commonly, aspergilloma may cause cough and fever.
Causes for Hemoptysis in Aspergilloma
- Incidence 55-87.5%; Massive haemoptysis: 10%
- Erosion of bronchial arteries; usually stops spontaneously
- Mechanisms: erosion of the vascular cyst wall by friction from the fungus ball, elaboration of endotoxin by the fungus, patient’s underlying disease, superimposed bacterial infection
- Neither the size, the complexity of the lesion, the presence of a warning minor haemoptysis, nor the type of underlying disease can predict those patients who will progress to life-threatening haemoptysis.
Aspergilloma as Post tuberculosis sequalae
- In our country tuberculosis is one of the most common predisposing factors.
- Commonest site – Upper lobes; Incidence – 0.16% – 17%
- The most common preceding lung lesion is an open healed tuberculosis cavity
- The incidence of cavitary TB being affected by aspergilloma is 11-17%.
- Interval between diagnosis of tuberculosis and development of aspergilloma may vary from less than a year to thirty years (Average is 9.2 years)
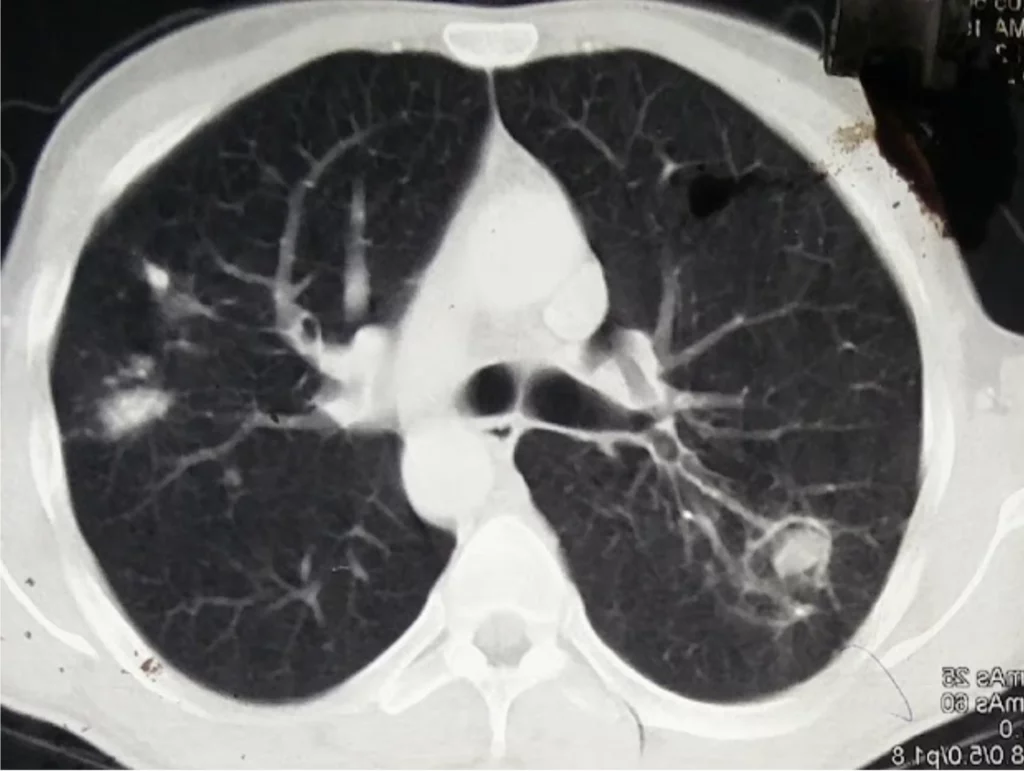
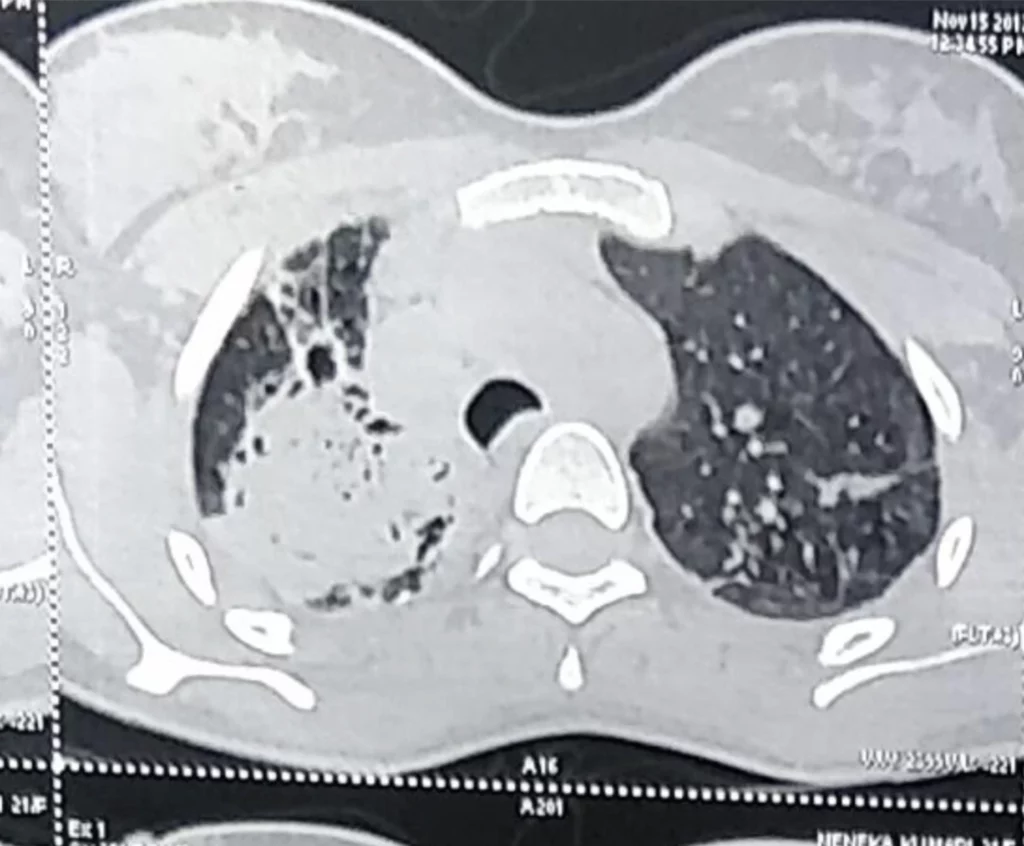
Radiological Findings
Radiographic and CT scan images may reveal characteristic patterns of aspergilloma, including nodules, cavitary infiltrates, and focal infiltrates . The characteristic chest radiographic appearance is that of a round or oval mass with the opacity of a soft-tissue mass. Often, an adjacent crescent-shaped air space (the air-crescent sign) separates the fungal ball from the cavity wall . The demonstration of a mobile mass within a cavity on supine and prone scans is virtually diagnostic of aspergilloma . CT scans better demonstrate these findings and can show the mobility of the mass between prone and supine positioning .
Simple Aspergilloma
- Cavity Characteristics:
o Typically found in a single, well-defined, thin-walled cavity.
o The cavity is usually isolated without significant communication with other lung structures. - Surrounding Lung Tissue:
o Generally normal or only mildly affected.
o There is little to no evidence of underlying lung disease, such as fibrosis or significant inflammation.
Complex Aspergilloma
Cavity Characteristics:
- Found in multiple or irregularly shaped cavities.
- The cavities may be thick-walled and interconnected, often resulting from more extensive lung damage.
Surrounding Lung Tissue
- Significant underlying lung disease such as chronic obstructive pulmonary disease (COPD), tuberculosis, sarcoidosis, or previous lung infections.
- Marked fibrosis, inflammation, or other structural lung changes are common.
Laboratory Tests
Certain laboratory tests aid in the diagnosis of aspergilloma and invasive aspergillosis. Serum and bronchoalveolar lavage (BAL) galactomannan measures are recommended as markers for the diagnosis of invasive aspergillosis . Polymerase chain reaction (PCR) assays can also be considered in conjunction with other diagnostic tests . In allergic bronchopulmonary aspergillosis (ABPA), prick or intradermal skin testing with Aspergillus antigen results in a positive reaction manifested by wheal and flare .
Procedures like bronchoscopy, needle biopsy, and open lung biopsy may be helpful for the diagnosis of invasive aspergillosis . At bronchoscopy, BAL in areas of pneumonia may provide evidence for the diagnosis, and transbronchial biopsy may be helpful . Histopathology and silver staining demonstrate the characteristic septate hyphae, branching at acute angles, and acute inflammatory infiltrate and tissue necrosis with occasional granulomata and blood vessel invasion.
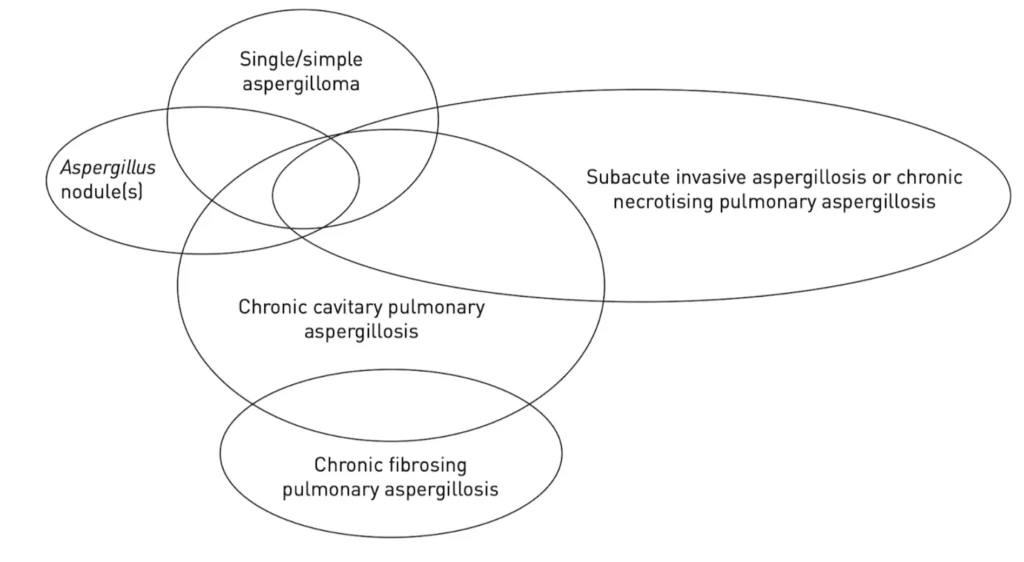
The diagnosis of CPA requires a combination of characteristics:
- Consistent appearance in thoracic imaging (preferably by CT)
- Direct evidence of Aspergillus infection or an immunological response to Aspergillus spp and exclusion of some alternative diagnoses
- In addition, by convention the disease will have been present for at least 3 months, even if that duration is inferred and based on symptoms or progressive radiological abnormality
Surgical Expertise for Aspergilloma in Delhi
Evidence for Surgery
Surgical resection of aspergilloma is a definitive treatment option for patients with adequate pulmonary function (SoR A and QoE II)
Success of the procedure depends on the ability to fully resect the aspergilloma without spillage of fungal elements into the pleural space.
According to IDSA guidelines, in patients at a low surgical risk, surgical resection can offer a permanent cure as well as avoid haemoptysis and locoregional extension, and therefore improves survival.
Choosing the Right Surgeon
Aspergilloma lung treatment in Delhi involves a multifaceted approach, with surgical intervention playing a crucial role in severe cases . Patients seeking Aspergilloma lung treatment in Delhi can benefit from the expertise of highly skilled thoracic surgeons who specialise in this complex condition . Dr Pallavi Purwar, possess extensive experience and a deep understanding of the intricate procedures required for the effective management of Aspergilloma.
- Not every Centre is equipped for Lung Resection in Aspergilloma
- Preoperative factors: Complex individual patient decisions in view of lack of standardised preoperative criteria for fitness ( when compared to lung cancer)
- Surgical Factors:
- Dense Adhesions, Calcified Lymph nodes, High likelihood of frozen hilum
- Higher likelihood of change in preoperative extent of resection in view of nodules or disease in other lung segments
- Postoperative factors: Higher risk for bronchopleural fistulae and complex management for such complications
- Institutional Factors: Team well trained in infection control
State-of-the-art Facilities
Leading medical facilities extended by Dr Pallavi Purwar in Delhi are equipped with state-of-the-art diagnostic tools, enabling precise identification of Aspergilloma and its extent in the lungs . These advanced imaging technologies, coupled with specialised surgical suites, provide an optimal environment for successful surgical interventions. Patients can expect to receive comprehensive care in our cutting-edge facilities, ensuring the highest standards of safety and efficacy.
Multidisciplinary Approach
In the realm of Aspergilloma lung treatment in Delhi, a multidisciplinary approach is often adopted, involving pulmonologists, infectious disease specialists, and respiratory therapists . This collaborative effort ensures a holistic and well-rounded treatment strategy. By combining the expertise of various medical professionals, patients receive personalised care tailored to their specific needs, maximising the chances of a successful outcome.
Thoracotomy, a surgical procedure that provides direct access to the affected lung tissue, is a crucial intervention for aspergilloma . During this surgery, Dr. Pallavi Purwar can accurately remove the fungus ball (mycetoma) and address any complications or lung damage . Thoracotomy offers an unobstructed view and precise maneuvering, making it an essential technique for successfully treating aspergilloma, restoring lung function, and improving the patient’s quality of life.
Preoperative evaluation and Fitness
- Blood tests: CBC, RFT, LFT, BS, SE, Coagulation Profile, viral markers
- Sputum-smear microscopy and culture with DST if prior TB
- Chest X-ray and CECT Thorax
- Fibreoptic Bronchoscopy especially if ongoing hemoptysis
- Pulmonary function test, Cardiac evaluation, V/Q scans Preoperative preparation
- Nutritional assessment and ABG
- Nutritional Rehabilitation
- Preoperative pulmonary rehabilitation and exercises
- No role of preoperative antifungals
- Smoking cessation
- Control of active hemoptysis by conservative or endobronchial therapy
Surgical Procedures and Outcomes
Types of Resections
Surgical resection is considered the gold standard treatment for aspergilloma, allowing for complete removal of the infected lobe and preventing recurrence . The choice of surgical procedure depends on the size and location of the aspergilloma lesion, as well as the patient’s lung capacity. For small lesions of 3 cm or less, a wedge resection or segmentectomy is typically performed . In cases of larger infiltration and sufficient lung capacity, a lobectomy is the preferred approach . In severe cases where the lung is severely damaged due to previous conditions like tuberculosis or scarring, a pneumonectomy (complete lung removal) may be necessary .
- Wedge/segmentectomy: Small simple aspergilloma
- either peripheral (wedge) or
- lies locally within a segment (segmentectomy).
- Lobectomy: Large simple aspergilloma or complex aspergillomas
- undesirable to leave diseased lung if patient can tolerate anatomical lung resection.
- may require tailoring the lobectomy to include a wedge of the adjacent lobe
- Pneumonectomy: Destroyed Lung, iatrogenic PA injury, Completion pneumonectomy
- Cavernostomy and limited thoracoplasty: high risk patients with complex aspergilloma: not tolerate anatomical resection
Postoperative care and challenges
- Preference to on table extubation
- Negative pressure chest drainage system for prevention of space problems
- Early resumption of deep breathing and respiratory exercises
- Vigorous monitoring of drain output following pneumonectomy
- Early Ambulation
- Normal diet and medications to be resumed as soon as feasible
Possible Complications
The most common complication is bleeding
- from twisted bronchial vessels, from aberrant systemic arteries growing close to the intercostals or internal mammary arteries, or from vascular adhesions resulting from chronic inflammatory pulmonary processes
The most dreaded complication is bronchopleural fistula
- bronchial weakness caused by chronic inflammation, atrophy, and calcification of the bronchial stump
- may lead to life- threatening complications such as respiratory insufficiency, empyema, and aspiration of purulent material to the healthy lung.
Persistent Air Leak
- 20-30% incidence
- Can be most often managed conservatively
Pleural space problems
- lung has lost elasticity because of different underlying disease (eg, sequelae of
tuberculosis or emphysema/fibrosis).
Success Rates
Surgical resection has been shown to greatly benefit patients who have experienced recurrent and significant hemoptysis (coughing up blood) associated with aspergilloma . Studies have reported a 5-year survival rate of 84% in patients who underwent surgical resection for aspergilloma with hemoptysis, compared to 41% in those managed with medical therapy alone . However, for asymptomatic patients, there was no significant difference in survival between surgical and medical management .
More recent studies have reported similar positive outcomes, with a 5-year survival rate of 85-93% after surgical resection for aspergilloma.
Postoperative antifungals
- Simple aspergilloma resected without spillage : no adjuvant antifungal therapy
- Intraoperative spillage: No consensus; we do not give; some advocate for 6 months
- Post-operative antifungal treatment may be considered
- cultures peri- or post-operatively are positive
- hyphae are seen in resected lung parenchyma (as opposed to the cavity);
- peri-operative difficulty in lesion removal with a risk of extension to contiguous lung segment(s) and/or pleura
- suboptimal surgery (residual lesions)
No recommendation: failure to completely resect the aspergilloma; individualised
Quality of Life After Surgery
Successful surgical resection of aspergilloma can significantly improve the patient’s quality of life by restoring lung function and preventing life-threatening complications such as massive hemoptysis, invasive aspergillosis, pulmonary fibrosis, or renal amyloidosis due to chronic inflammation . Thoracotomy, a surgical procedure that provides direct access to the affected lung tissue, is crucial for accurately removing the fungus ball (mycetoma) and addressing any lung damage . This technique offers an unobstructed view and precise maneuvering, making it an essential approach for successfully treating aspergilloma and improving the patient’s overall well-being. However Dr Pallavi offers minimally invasive (VATS ) surgery for all simple aspergilloma and select complex aspergilloma cases.
After surgery, the recurrence rate of hemoptysis is low, and the recurrence rate of pulmonary aspergilloma is reported to be around 5-7%, which is most commonly due to insufficient extent of parenchymal resection, the presence of additional lung cavities, and continued immunosuppression .
Conclusion
Aspergilloma lung treatment in Delhi has made significant strides, offering hope to patients grappling with this complex fungal infection. The combination of expert surgical skills, cutting-edge facilities, and a team-based approach has a profound influence on patient outcomes. These advancements not only improve survival rates but also enhance the overall quality of life for those affected by this challenging condition.
Looking ahead, the future of aspergilloma treatment in Delhi seems promising. As medical knowledge grows and surgical techniques continue to evolve, patients can expect even better results and fewer complications. This progress in treating aspergilloma serves as a beacon of hope, highlighting Delhi’s position as a key player in tackling complex respiratory conditions and offering top-notch care to improve lung health.
FAQs
1. What type of surgery is performed for fungal infections in the lungs?
Surgery is the primary treatment option for aspergillomas, which are fungal masses in the lungs, especially when they cause bleeding. Since antifungal medications are not very effective at reaching the aspergilloma, removing the fungal mass surgically is often necessary. Additionally, embolization may be used to halt lung bleeding caused by an aspergilloma.
2. Is it possible to surgically remove a fungus from the lungs?
Yes, surgically removing a fungal ball from the lungs is often the best treatment for patients with chronic pulmonary aspergillosis, particularly when the mass is located in an accessible area. Antifungal medications are generally less effective for these conditions.
3. What does surgery for pulmonary aspergilloma entail?
The surgical approach for treating pulmonary aspergilloma involves removing the fungal ball and the underlying cavity along with any diseased lung tissue. This procedure aims to prevent severe complications such as life-threatening bleeding, invasive aspergillus disease, pulmonary fibrosis, or renal amyloidosis, which can arise from chronic inflammation.
4. What is an aspergilloma?
An aspergilloma, also known as a fungal mass, is a clump of fungus that forms within a lung cavity. These cavities often develop as a result of prior lung conditions, with tuberculosis being a common cause.
Book Consultation
Reach us as per the contact details provided on the website to book your appointment.
Achievements
- 10+ Years of Experience
- Robotic Surgery: State-of-the-art technology
- VATS: Video-assisted thoracic surgery – Keyhole surgery
- Chest Surgery: Various benign and malignant diseases of lungs
- TB Surgery: Surgical treatment of complications of pulmonary tuberculosis
Why Choose Dr. Pallavi Purwar
- Specialised Expertise
- Patient-Centered Approach
- Comprehensive Care
- Highly Experienced
- Better Patient Outcomes
Contact Information
- Email: [email protected]
- Phone: +91 99100 81862